‘Practical Interoperability’ means different things to different healthcare stakeholders. In the HealthCare Executive Group’s first Focus Area Roundtable on Interoperability, leaders associated with health plans, care providers, and organizations supporting the healthcare system discussed what practical interoperability means to them. Addressing barriers to interoperability and use cases with the most potential to increase interoperability was a primary focus of the roundtable with highlights shared in the first post recapping the roundtable titled ‘Discussing Barriers to Healthcare Interoperability, Use-Cases, and More.’ This second post shares additional highlights including increasing adoption of use cases, the importance of trust among stakeholders, interoperability’s increasing impact on value-based arrangements, and workflow considerations – particularly in terms of balancing the amount of information exchanged by payers and providers.
Read Part 1 of the recap of this first Focus Area Roundtable on Interoperability here.
Importance of Establishing & Maintaining Trust to Overcome Barriers to Practical Interoperability
Building on discussion of the importance of health plan-provider collaboration and which stakeholders are best positioned, qualified, and equipped to own specific interoperability use cases, HCEG’s Ferris Taylor noted the abundance of EMR’s, robust data sets that increasingly include structured clinical data, and analytical capabilities that weren’t available 12-15 years ago. These data and analytics, along with mandates on transparency and interoperability – particularly electronic prior authorization and pricing data – are forcing stakeholders to increase trust among themselves and other 3rd parties.
Ferris asked Tim Capstick, Regional Vice President of Health Plans at Surescripts, to frame the discussion of developing trust to unlock the value of increasing practical interoperability.
Developing a Trust Framework to Unlock the Value of Existing Healthcare Data Assets

Tim set the context for roundtable comments by sharing how well-defined standards, clearly understood use cases, and trustworthy partners serve as the essential foundation to maximize business model benefits of increased interoperability. Tim emphasized: “We have to be able to trust whoever’s going to sit in the middle – or bring these entities together. We’ll have to be able to trust each other and make sure that we know and trust what each other are going to be doing with this information.”
Listen here for more on establishing trust to unlock the value of healthcare data
RELATED: Building Trust is Essential to Transforming the Healthcare System
Establish Trust by Consistently Providing Quality Information That Returns Value
One participant representing a research organization shared that standards – particularly FHIR – will help with advancing practical interoperability once the data content, elements and formats of these standards are better understood.
Participant Denny Brennan, Executive Director and Chief Executive Officer of HCEG partner Massachusetts Health Data Consortium (MHDC), weighed in on the importance of by sharing that MHDC is creating an implementation guide combining DaVinci-compatible payer data and clinical data exchange standards related to prior authorization.
Denny noted that payers and providers have a great deal of work getting their digital house in order and making the necessary data available to accelerate instantaneous or close to instantaneous prior authorizations for services that today are difficult, arduous, and don’t require a huge amount of clinical intervention, if anything, to make the decision.
Listen here for more on the importance of providing quality data to healthcare providers
See Price Transparency Data Standards & Operational Considerations from a recent roundtable in Price Transparency facilitated by our Focus Area Partner HealthSparq.
Balancing Amount of Data Shared with Providers – Increasing Impact of Value-based Arrangements
Other discussions involved challenges, issues, and opportunities regarding interoperability’s impact on the day-to-day workflow of healthcare stakeholders – particularly in terms of how care providers are accessing information and what information is being presented. The balance between providing too much information that can overwhelm care providers, administratively burdens them, and inhibits their ability to do what they need to do and responding to provider requests for more information to make care decisions were discussed. Participants noted value-based arrangements and risk-based reimbursement models are clearly an impetus for increased interoperability and drive desire from the provider community for more information. Being mindful of the process workflow of care providers, what information is inserted into the workflow, and how that information is inserted and accessed was identified as key considerations.
RELATED: How Health Plans Can Best Support Provider Organizations Address Barriers to Practical Interoperability
The Importance of Breaking Workflow to Include Business Partners
Roundtable participants made clear that accommodating care provider information demands – whether under traditional FFS or new value-based payment models – requires a thoughtful change to provider workflows. In addition, compliance with interoperability mandates and realizing practical interoperability’s greater benefits means all stakeholders will need to break their routines and [modify] their workflows to include partners.
“Stakeholders don’t have to do this themselves if they can get out of the adversarial zero-sum game that, if we share data with providers, or we share data with health plans, they are going to use those data against us or whatever scenario comes to mind. There’s a lot of money that’s being swept off the table by IT vendors who are offering niche services that ultimately never get used.” – Roundtable Participant
As shared in the Part 1 recap of the roundtable on interoperability, if providers invested in better collaboration with their payers, they might reduce their investment in the technologies to support processes they thought they were going to do entirely by themselves.
Listen here for more on breaking business partner workflow to reduce overall IT investments
Interoperability Vendors Serving the Healthcare Market – a Darwinian Experiment
Participants shared various comments about increasing the adoption and evolution of interoperability-related initiatives, programs, and applications.
One participant shared his observation that, on the intervention side, increased interoperability is empowering many great third-party companies that are already doing great work around mobile engagement, disease management, and so on.
“There’s a whole bunch of them. There’s been a sort of Darwinian experiment of all these different vendors about what approaches to take and we’re starting to see some rise to the top; to create the ability for them [providers] to sort of socket in a secure way and play on the platform and do things for the benefit of patients.”
Another shared that healthcare stakeholders have a collective obligation to create a competitive environment for the adoption of practical interoperability:
“I think when we talk about interoperability, we have just not a responsibility but really an obligation to create a competitive environment where they can come and play and let the best continue to rise to the top.”
And another shared a suggestion to healthcare providers who think they can avoid sharing their healthcare data.
“One of the steps that we have to really focus on in terms of what do payers and providers have to do is: stop thinking you have to do everything yourself. You’re going to have to share data. Forget about arguing about that. Forget about it. You’re going to have to share everything. The deal is done. It’s over. You’re going to have to be transparent, get over it, stop complaining about it.”
And now, healthcare requires payers and providers are going to have to really start thinking about creating new, collaborative business models that engage consumers. And if they don’t do that and each go after the consumer in their own way, they’re just complicating the problem we have today which is: I want to go to one place to get all my health data. The fact that it’s a health plan as envisioned in the regulation should not preclude any progress.
Quality Measures: Data Requirements, Costs, & Impact of Upcoming Changes
A participant from a small health plan noted the number of new hybrid measures related to telehealth services and how interoperability mandates and related initiatives will impact provider collection of quality measures and submission to health plans; particularly as the CMS deadline for transition to all-digital quality measures takes place in 2025 and information currently being collected goes away.
Sharing Information – It’s the Law & The Right Thing to Do
This participant representing a small health plan expressed concern about the number of EMR systems in use at health systems, the overall lack of awareness, understanding and adoption of interoperability mandates among the provider community, and the challenges that present health plans – particularly smaller health plans – with accessing data from health systems.
She mentioned the cost impact of both complying with interoperability mandates and how some providers and health systems charge for access to data housed in their individual EMR’s.
“We’re sitting here knowing that our entire world is going to digital, knowing that we have to get to digital, seeing interoperability as one opportunity for everybody collectively to get to digital. But the adoption rate is The Big Question in my mind.”
Listen here to the leader of a small health plan share insight on accessing data
Information Blocking – Serious Consequences for Non-Compliance
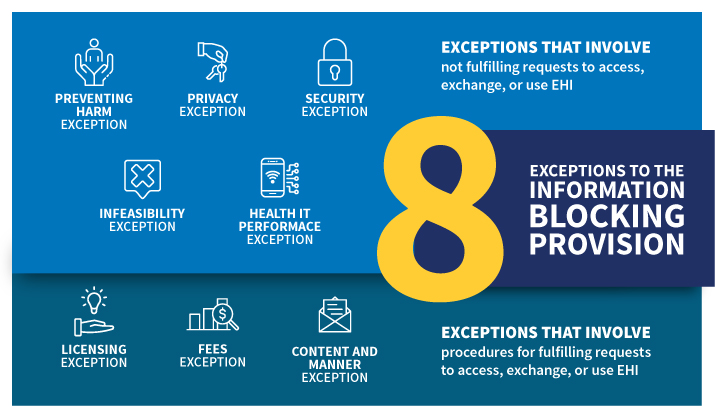
Source: Office of the National Coordinator for Health Information Technology (ONC)
Existing regulation concerning Information Blocking (Section 4004 of the 21st Century Cures Act) was raised with one participant noting that charging fees for accessing, exchanging, or using Electronic Health Information (EHI) – with exception per 45 CFR § 171.302 – is a felony. He noted that while a smaller subset of EHI data (elements defined in USCDI Version 1) is currently subject to Information Blocking through October 5th, 2022, regulations expanding those data elements to USCDI version 2 are quickly approaching and the regulated community should make all EHI available as if the scope of EHI were not currently limited to Version 1.
Patience for Non-Compliance with Information Blocking Regulations is Decreasing
This topic of discussion was ended with this participant saying:
“And CMS and the [Biden] Administration have shown absolutely no patience whatsoever with that stance. So, I think health plans who were finding themselves running up against EMR’S who are trying to monetize data and the availability of data from their records, have the weight of the law behind them. Providers who try to monetize their data exchanges with health plans directly is not okay unless it’s purely at cost or something very close to at cost if it’s an extraordinary effort. And going forward it’s not going to command a very high premium to get data from the provider who’s treating a member.”
Listen here to a healthcare data expert on provider reluctance to share data with health plans
Learn More About Practical Interoperability

On September 8th, 2021, leaders of health plans, health systems, and provider organizations will have the opportunity to discuss the real-life initiatives, programs, applications, and technologies their organizations are considering, implementing, or currently using to address the challenges, issues, and opportunities recapped here and in the first post of this two-part series. Leaders of health plans, health systems, and provider organizations are encouraged to request an invite here.
Special thanks to Ashley Clark and Tim Capstick of our sponsor Surescripts for sharing their unique insight in this roundtable. For information on any of the topics presented in this post, contact Tim Capstick or Ashley Clark.
To receive additional information on interoperability and other healthcare leader priorities presented on the 2021 HCEG Top 10+ list, subscribe to our newsletter and follow us on Twitter and LinkedIn.



